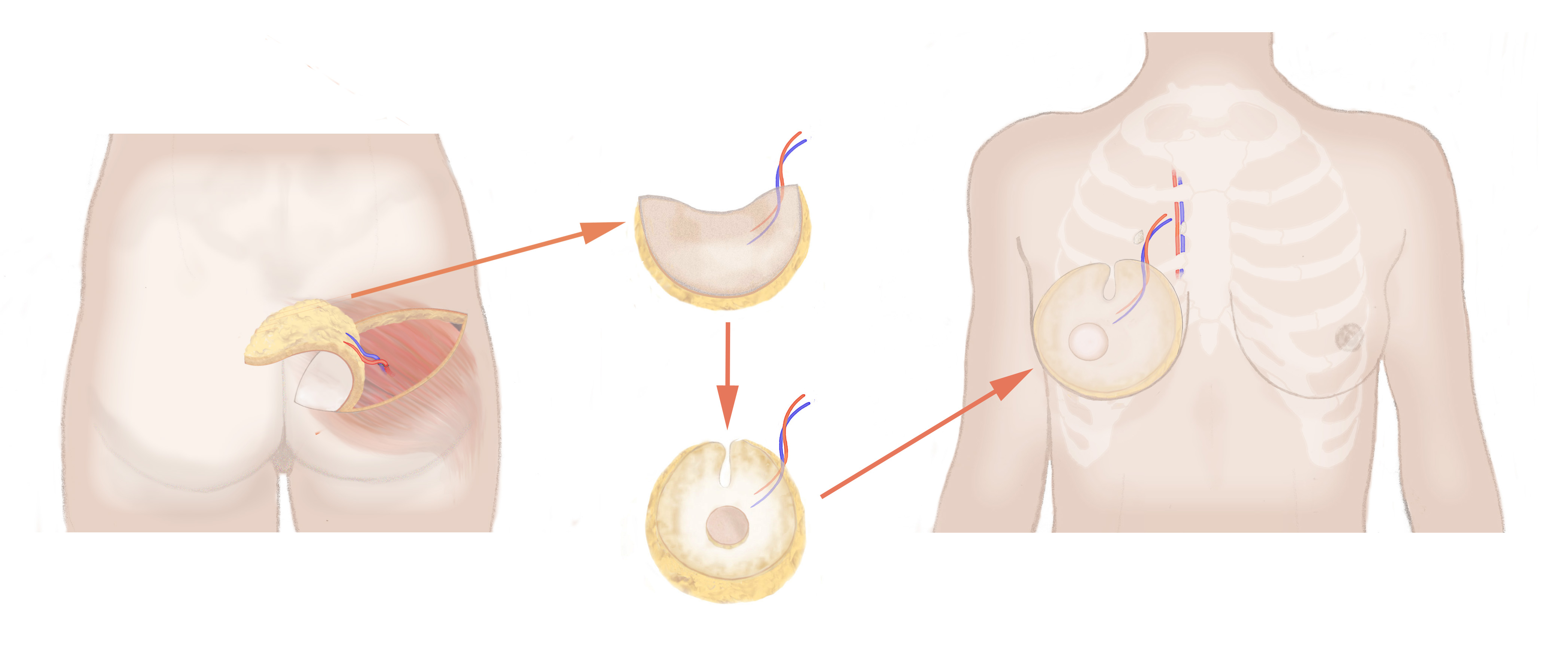
| What is an SGAP flap? Some women who request autologous breast reconstruction (using their own tissue), are too slim and do not have enough fat tissue in the lower abdomen to perform a DIEP flap. Others may have had a surgical procedure in the past to the abdomen, which has led to scarring. These women may be able to have an SGAP procedure performed instead. With the SGAP, or Superior Gluteal Artery Perforator flap, excess skin and fat from the upper buttock region is taken without any muscle and transferred as a free flap to the chest to create the new breast. Microsurgical techniques are used to reconnect the blood supply |
|
| What is the difference between the SGAP and the DIEP? Both flaps are perforator flaps – they both use tissue consisting only of skin and fat without any muscle. One of the differences is that the tissue used for the SGAP flap is more compact than with the DIEP. Another important difference is that patients undergoing an S-GAP flap procedure recover more quickly than those with a DIEP flap. |
| What risks are associated with the SGAP flap procedure? It is technically more challenging to raise SGAP tissue than DIEP flap tissue. The vessels are smaller and the anatomy more unpredictable. Therefore, the failure rate is slightly higher. However, problems occurring at the donor site (other than a small amount of asymmetry) are rare. |
| Will there be a significant asymmetry? According to patient surveys, most women haven\’t noticed significant asymmetry (i.e. visible through their clothing). |
SGAP flap – overview |
|
| Operation time: | 5-8 hours |
| Hospital Stay: | 4-5 nights following the operations |
| Type of Anaesthesia: | General anaesthetic |
| Recovery Time: | Around 3 Weeks |
| Risks of Surgery include: | Bruising, swelling and discomfort.
In rare cases, patients experience bleeding (haematoma), infection, failure of the flap (approx 4%), partial failure of flap, the need to re-operate (approx 8%), wound breakdown or necrosis of the mastectomy skin flaps. Problems occurring a week after the operation can include reduced sensation of reconstructed breast. Other (rare) problems can include scarring, an unsightly, lumpy breast; asymmetry of the buttock; seroma |
| Further Treatment: | Visit to the Hospital Dressing Clinic (a week after discharge) |
| Nipple reconstruction: | Around 3 months later |
| Nipple Tattooing: | 1 month after reconstruction (by your surgical team) |